Abstract
Tuberculosis and female reproductive health
Tuberculosis (TB) is an important cause of mortality and morbidity all over the world and is particularly relevant in developing countries like India where the disease is endemic. Female reproductive system is very vulnerable to this infection and clinical presentation of this disease in a large majority of patients could be completely silent. This disease is an important cause of infertility, menstrual irregularity, pregnancy loss, morbidity to both the mother and child increases in pregnancy. The clinical diagnosis of genital TB requires a high index of suspicion. Approximately 50% of patients might have had tuberculous pleurisy, peritonitis, or renal, osseous, or pulmonary TB. A history of primary infertility in a woman in whom examination reveals no apparent cause and who gives a family history of TB should arouse suspicion .A history of poor general health associated with weight loss, undue fatigue, low-grade fever, or vague lower abdominal discomfort is often elicited in patients The diagnosis of TB is based on the identification of M. tuberculosis or others of the M. tuberculosis complex in culture. Other tests include Complete blood count, Chest radiographs,Tuberculin test, Menstrual blood for culture, Endometrial curettage-histologic examination, Hysterosalpingography, Ultrasonography etc . Treatment includes a 6-month regimen consisting of isoniazid (INH), rifampin (RIF) and pyrazinamide (PZA) for 2 months, followed by INH and RIF for 4 months. It is a global health priority that tuberculosis treatment be made available to women, particularly to those in low-income countries who are bearing the brunt of this epidemic.
Author(s): Tanvi Tuteja
Abstract | Full-Text | PDF
Share this

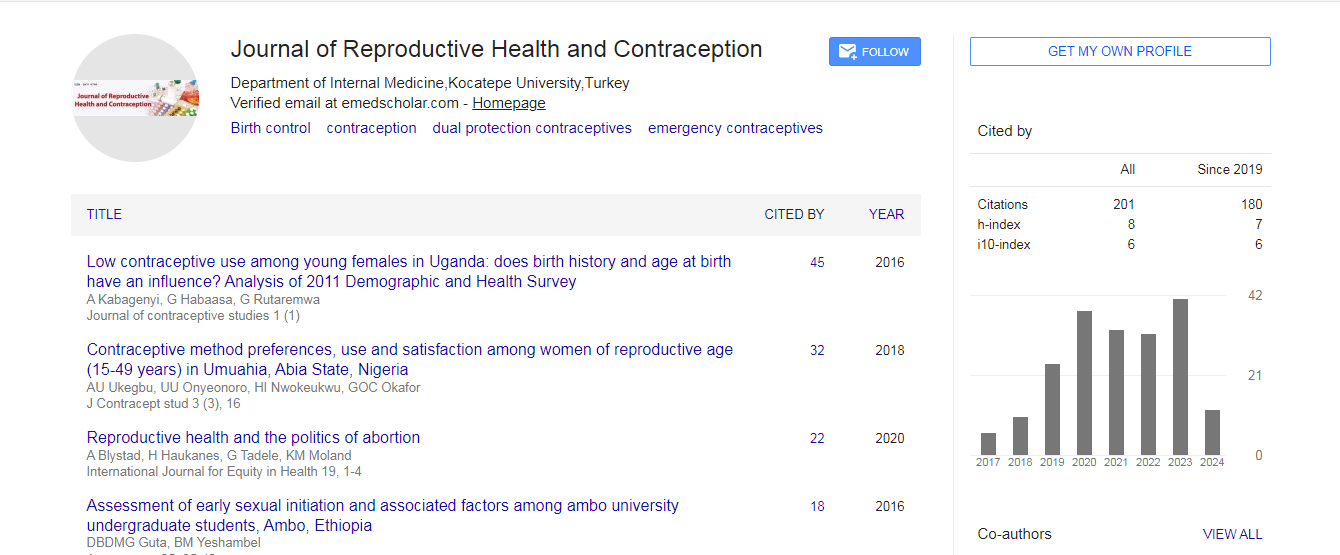
Google scholar citation report
Citations : 201
Journal of Reproductive Health and Contraception received 201 citations as per google scholar report
Journal of Reproductive Health and Contraception peer review process verified at publons
Abstracted/Indexed in
- Google Scholar
- China National Knowledge Infrastructure (CNKI)
- WorldCat
- Publons


Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences